Check if Move is covered for you

The Sword Summary Warm-up
Here are the key takeaways:
- A Saxenda plateau does not mean the medication has stopped working. It reflects a metabolic shift that most people on GLP-1s never address.
- Lean muscle loss during treatment quietly lowers resting metabolic rate, stalling the scale even when you are following your plan exactly.
- The longer you have been on Saxenda without structured movement, the more lean mass you have likely lost. Saxenda's daily dosing means this risk accumulates faster than with once-weekly GLP-1s.
- Cutting calories further deepens the plateau. Preserving muscle is the lever that breaks it.
- Sword Move provides structured, clinically guided movement designed to preserve and rebuild lean mass so the scale can start moving again.
If you have hit a plateau on Saxenda, you are probably not a beginner. You have been on it for months. Appetite under control. Routine locked in. The scale was moving. Then, somewhere around week eight or ten, it stopped.
The frustration is different from how it felt when you first started. You have lived through real change. You have seen the results. You know how the medication works. So when progress stalls, it does not feel like a beginner's stumble. It feels like something that was working has quietly broken.
This is a common experience, and the reason the scale has stalled is likely specific. The fix most people reach for can actually make things worse. Here is what to do instead.
Saxenda is still working, but your metabolism can hit a ceiling
Saxenda contains liraglutide, a GLP-1 receptor agonist (a type of medication that reduces appetite and slows digestion). Reducing caloric intake drives the early weight loss. What the medication cannot control is what happens alongside that calorie reduction.
When you eat less, you often move less too. Not just during exercise. Throughout the whole day. Fewer steps between tasks, less energy for small physical demands that add up: incidental movement drops alongside caloric intake, and most people never notice it happening.
Without movement to counterbalance this, the body draws on both fat and lean muscle for energy. Muscle is metabolically expensive to maintain: the more of it you carry, the more calories your body burns at rest. Lose it, and resting metabolic rate falls with it. The scale stalls not because Saxenda stopped working, but because the engine driving caloric burn has downshifted.
Up to 39% of lean body mass can be lost during GLP-1 use, particularly in people who are not regularly active.¹ That figure shows why people following their plan to the letter can still hit a plateau many months into treatment.
Why people on Saxenda face this sooner than most
Liraglutide has a 13-hour half-life and is injected daily. People on Saxenda typically stay on it for longer continuous stretches than people on once-weekly GLP-1s like semaglutide.²
The practical result: lean mass loss accumulates for longer before anything changes. Someone at month eight of Saxenda treatment is managing significantly more metabolic adaptation than someone at month two. The plateau does not sit still. It deepens as time passes.
Why eating less makes the plateau worse
Restricting calories further when the scale stalls is the intuitive response. It is also the one most likely to deepen the problem.
Cutting intake without adding movement accelerates lean mass loss. Less muscle drives resting metabolic rate lower, which means the body needs even fewer calories to hold its weight. Each round of restriction tightens that ceiling further. The body adapts faster than the scale moves.
The plateau is a body composition problem: the fat-to-lean ratio has shifted in the wrong direction, and caloric arithmetic cannot fix that. More restriction presses on the wrong variable, accelerates muscle loss, and leaves progress harder to rebuild than if you had not restricted further at all.
Strength training is what actually changes the equation
The effective intervention is structured, resistance-based movement. Not extra cardio. Not chasing step targets. Resistance training signals the body to preserve and rebuild lean muscle rather than shed it.
More muscle raises resting metabolic rate. Progress shifts away from scale weight and toward body composition: less fat, more lean tissue. The scale may move more slowly, but what moves is fat rather than muscle. That distinction compounds over months and makes results easier to sustain.
Getting started does not require a gym or an existing fitness habit. Resistance bands, bodyweight exercises, or light free weights; 20 to 30 minutes per session, three to four times per week; at home, at any fitness level. That is the minimum effective dose. It is enough to change what the body prioritises when it is in a caloric deficit.
Planning to switch medications? Start movement now, not after
Some people reading this are also considering a switch to a newer once-weekly GLP-1, or planning a break from medication entirely.
The body composition math applies regardless. Lean mass built before a transition carries forward to any new medication. Lean mass lost before that transition is a deficit any new prescription inherits. Switching to Ozempic will not restore muscle lost on Saxenda. The same is true of Wegovy and Mounjaro. Only structured movement does that.
Starting before a medication change, not after settling into a new one, is when movement intervention delivers the most value. For more on managing that transition, see stopping Saxenda and keeping the weight off.
Getting started is the hardest part
Understanding the mechanism is one thing. Building a consistent movement routine after months of lower activity is another, especially when energy is unpredictable and the scale has been discouraging. That is where structure matters most.
Sword Move provides structured, clinically guided movement for people managing weight and metabolic health. Each member works with a physical health specialist who holds a doctor of physical Therapy degree, builds a personalized plan, and adjusts it as strength improves. Sessions run 20 minutes or less and can be completed at any time, from anywhere. Each member receives a Move wearable, or can use their own connected device, to track progress in real time, with regular check-ins to keep the plan calibrated.
Get started with Sword Move for whole-body strength
1. Tell us about you
We’ll learn about your goals, job type, lifestyle, and movement history.

2. Match with a Physical Health Specialist
Your dedicated Sword Move specialist will create a personalized plan just for you.

3. Receive your Move kit
You’ll get a free Move wearable and resistance bands delivered to your door.
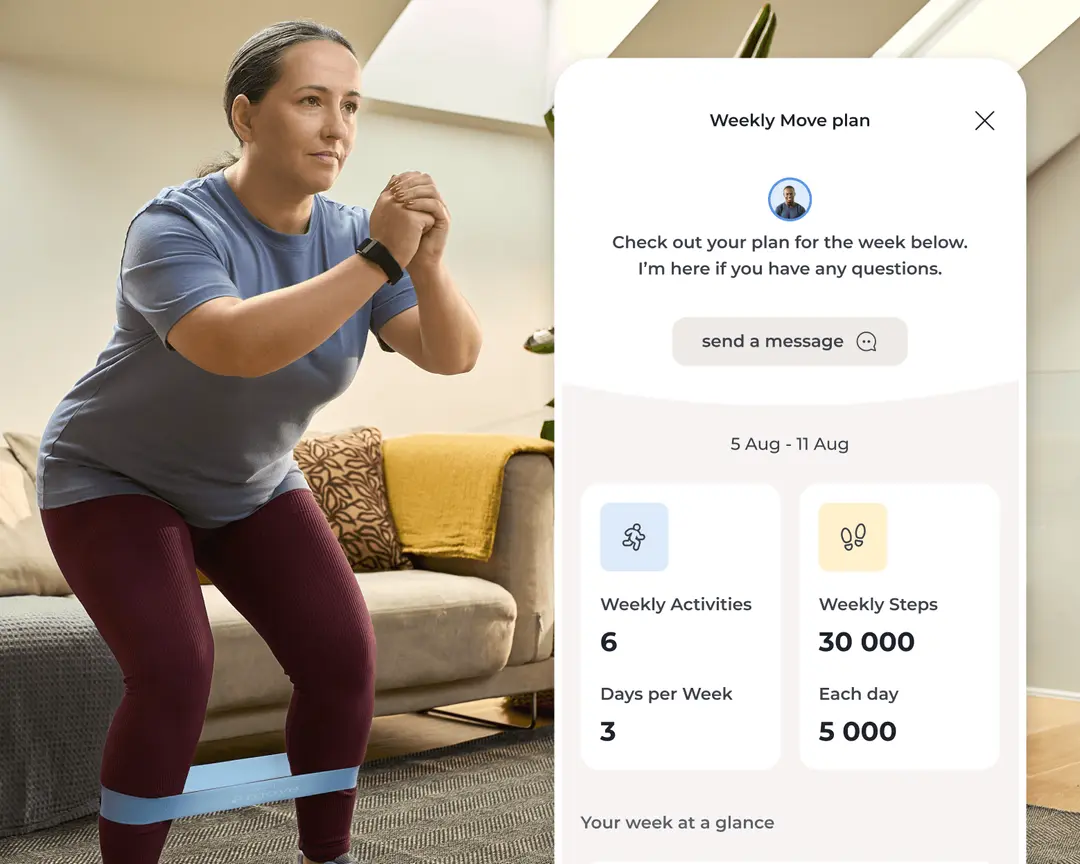
4. Start moving with your personalized plan
Pair your Move wearable and begin weekly goals built around your activity level, routines, and progress.
Among members who began from low activity levels:
- 69% reached "active" or "healthy active" status within 10 weeks³
- Members completed an average of 4.5 sessions per week⁴
- Sedentary time fell by 1 hour and 22 minutes per day for previously inactive members⁵
Functional shifts in how the body moves and burns energy. The kind that change the body composition numbers stalling the scale.
Progress starts with what Saxenda cannot provide
The medication is doing its job. The body composition shift that stalls the scale is the part a GLP-1 cannot fix on its own.
Add structured movement, and the plateau breaks. Muscle is preserved. Resting metabolic rate stabilises. The scale starts reflecting what the medication was always capable of delivering.
Sword Move may already be covered in your health plan at no out-of-pocket cost. Check your eligibility to find out if you can get started right away.
About the author

Sword Editorial Team
Evidence-based healthcare insights