The hidden healthcare costs of GLP-1s
GLP-1 medications like Ozempic and Wegovy are transforming how employers approach obesity care. Once reserved for diabetes patients, these drugs are now widely prescribed for weight loss. GLP-1 drugs do deliver on their promise of improved cardiometabolic outcomes. Simply, these medications do help users lose weight.
But for health plans and employers, the real challenge goes beyond pharmacy claims. The bigger risk is in the hidden costs that accumulate over time when GLP-1 treatment is not paired with sustainable lifestyle support. Without support to protect lean muscle, maintain function, and build healthier habits, employers may face a second wave of musculoskeletal claims, re-prescriptions, and disability-related costs.
GLP-1 users often do not develop the strength, nutrition, and day-to-day lifestyle habit changes needed to sustain results over time. Research also suggests that a meaningful share of weight lost during GLP-1 use may come from lean mass, which can leave people with lower strength and stability if that loss is not addressed.⁵
GLP-1s are effective, but expensive
One of the biggest concerns with GLP-1 use is sustainability. Many patients rebound to old habits after stopping treatment. GLP-1s are clinically effective for weight loss, but their price tag is steep. GLP-1s can cost up to $10,000 per member annually¹, and are projected to account for up to 9% of total medical spend² in some employer plans. The ROI, however, is not guaranteed.
- up to 70% of GLP-1 users discontinue medication within the first year³
- as many as two-thirds of patients regain weight after stopping⁴.
- clinical research shows that up to 39% of weight lost comes from lean mass⁵, not fat.
That can create new risks related to strength, stability, falls, and functional decline. GLP-1s are effective at driving weight loss, but without parallel support that helps members preserve muscle and maintain function, those gains can come with downstream healthcare costs.
Breaking down the cost burden of GLP-1s for employers
At first glance, GLP-1 adoption appears to reduce downstream spend by improving metabolic health. But a closer look shows additional cost centers that often go unreported:
- High churn risk: 30–50% of users discontinue within a year³, leading to rebound and re-prescription.
- No wraparound support: Without structured support for movement, nutrition, and daily habits, GLP-1 users may not develop the routines required to sustain weight loss over the long term.
- Functional degradation: Lean muscle loss and inactivity increase the likelihood of MSK claims and disability risk.
- Absence of ROI tracking: Many employers lack visibility into whether GLP-1s actually reduce long-term claims.
The result is high upfront pharmacy spend with unclear long-term return. Employers must look beyond GLP-1 medication costs alone to see the full financial picture of their investment. By pairing GLP-1 coverage with structured wraparound support, employers and health plans can improve the odds that early medication results translate into healthier long-term outcomes and more defensible financial performance.
Why pharmacy spend is only the beginning of your GLP-1 cost center
Even with careful formulary controls, GLP-1 costs don’t stop at the prescription. The real price often shows up in the months and years that follow. Most of these costs never show up under a GLP-1 code and that’s why a more complete lens is needed to maximize return on investment.
Raw claims data often doesn’t reveal the muscle loss, MSK risk, and productivity losses that can come from GLP-1 patients as a result of Sarcopenia, or lean muscle loss.
Clinical studies show that up to 39% of weight lost during GLP-1 use is lean muscle mass⁵. This is not just a cosmetic concern. Muscle plays a central role in protecting members from costly conditions:
- It drives metabolism and glucose control⁶
- It protects joints and reduces MSK stress⁷
- It supports balance, mobility, and independence⁸
When muscle is lost, members become weaker, less stable, and more vulnerable to MSK issues. This cascades into real costs for employers. Research links sarcopenia to:
- 33% of chronic pain cases in older adults⁹
- 60% higher risk of falls¹⁰
- 2.5x greater disability risk in people with sarcopenic obesity¹¹
These outcomes lead to rising MSK claims, rehab referrals, disability filings, and ultimately higher healthcare spend.
Inactivity increases MSK risk for GLP-1 users
There's one significant additional challenge that threatens the success of long-term weight loss: many members begin treatment from a low-activity baseline. According to the CDC, fewer than 1 in 4 U.S. adults meet physical activity guidelines¹². That means many GLP-1 users may already lack the strength and activity habits needed to preserve muscle during weight loss. Sword's Pulse member base reflects this reality:
- 76% are overweight or obese¹³
- 57% have an addressable health condition such as diabetes, high cholesterol, or a similar condition¹⁴
- 46% had low physical activity at baseline¹⁵
These are exactly the populations most likely to need more than a prescription alone. Employers that cover GLP-1s without structured support risk higher downstream claims, reduced durability of outcomes, and avoidable repeat spend.
Lifestyle support is the multiplier for GLP-1 success
GLP-1s suppress appetite, but they do not build muscle, improve function, or create lasting habits on their own. Structured support helps fill that gap. Movement is part of that picture, but so are nutrition guidance, habit formation, and support that continues between clinical touchpoints. Evidence suggests these elements matter when the goal is not just weight loss, but outcomes that hold over time.
- Help members preserve lean mass during weight loss⁵
- Support strength, mobility, and function during body-composition change⁹ ¹⁰
- Improve the odds that early progress becomes sustainable over time⁴
- Reinforce the daily habits that medication alone does not create
Sword Pulse is specifically designed to support GLP-1 users with the guidance and expertise they need to sustain healthy long-term weight loss.
Pulse members who begin with low activity levels show early signs of engagement that matter for long-term sustainability:
- 83% of Pulse members report feeling better or much better¹⁶
- 51% of members with low physical activity at baseline reached the World Health Organization’s recommended activity threshold after 27 days of Pulse sessions¹⁷
These signals do not prove every downstream financial outcome on their own. But they do show the kind of sustained engagement employers need if they want GLP-1 coverage to produce more durable results over time.
How Pulse can lower the total cost of care for GLP-1 users
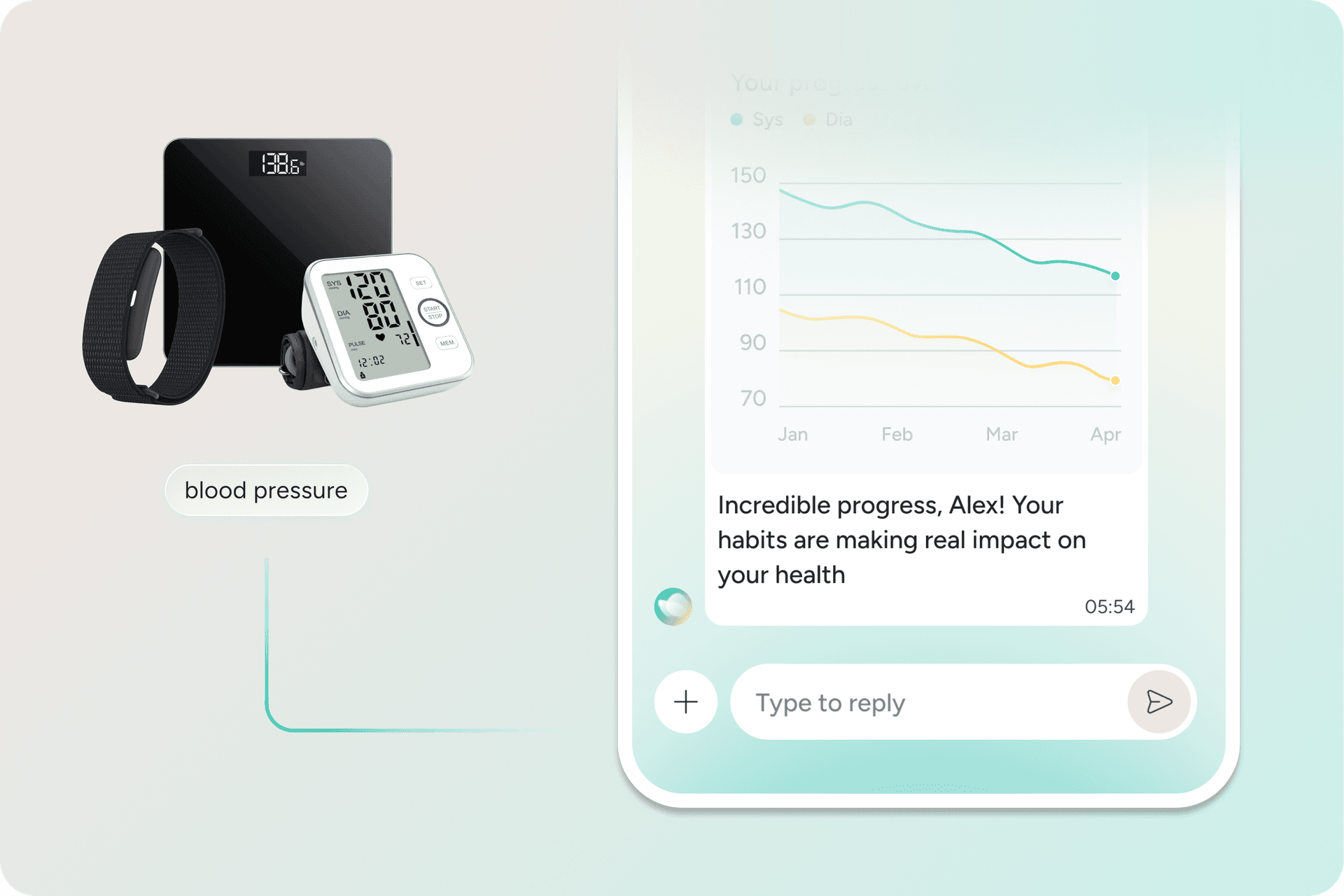
Pulse is the cardiometabolic pillar of the AI Care Platform, designed to support people managing blood pressure, blood sugar, cholesterol, weight, and GLP-1 use through continuous lifestyle support. For GLP-1 users, Pulse is built to address what medication alone does not:
- strength building to protect muscle
- nutrition guidance to preserve long term results
- developing the day-to-day lifestyle habits needed to sustain weight loss ¹⁸ ¹⁹
Pulse combines Phoenix, Sword Health’s AI Care Specialist, with guidance from a Health Specialist and connected devices that bring objective health data into each interaction. Instead of relying on episodic check-ins, Pulse provides ongoing support that adapts over time to what is actually working for the member.
How Pulse supports more sustainable GLP-1 outcomes
Pulse provides GLP-1 wraparound care that helps members preserve muscle, build strength, and develop healthier routines alongside medication use. The goal is not to replace the prescription. It is to support the parts of the journey medication does not cover on its own.¹⁸ Each Pulse member receives:
- Personalized support across movement, nutrition, and daily habits
- Ongoing engagement from Phoenix, Sword Health’s AI Care Specialist
- Guidance from a matched Health Specialist when nuance or clinical judgment matters
- Connected-device support, including blood pressure monitors, smart scales, and wearables where appropriate
- Reporting tied to engagement and measurable improvement
This kind of continuous support is especially important for GLP-1 populations, where success depends not only on weight loss, but on whether members maintain strength, function, and habits over time.
Use Pulse to strengthen the value of your GLP-1 strategy
GLP-1s can be effective at helping members lose weight, but they are rarely a standalone solution. Employers that cover GLP-1s without structured wraparound support risk weaker long-term durability, repeat spend, and additional downstream costs.
Pulse helps address that gap through continuous cardiometabolic support designed to preserve muscle, reinforce healthy habits, and keep members engaged over time. Pulse also delivers a 3.1x ROI validated by the Validation Institute and $1,663 in average annual savings per member.¹⁸ ¹⁹
About the author

Morgan Hollis
Head of Clinical Strategy, Sword Pulse