Check if Move is covered for you

The Sword Summary Warm-up
Don’t have time for the full workout? We’ve got you covered with a quick, high-intensity session. Here are the key takeaways:
- All GLP-1 and GIP/GLP-1 medications can lead to meaningful muscle loss during weight reduction.
- Research shows that 20 to 50 percent of the weight lost on these medications may come from lean mass, which includes muscle.¹
- Muscle is essential for metabolism, joint protection, balance, and long-term health.
- Protecting muscle requires supporting structured movement plans alongside GLP-1 prescriptions to sustain healthy fat loss.
Move, Sword Health’s personalized whole-body movement program, makes protecting your muscle strength easy. You can complete your exercises at any time, from the comfort of home.
What part of GLP-1 treatment do too many people overlook?
GLP-1 and GIP/GLP-1 medications like Ozempic, Wegovy, Mounjaro, and Zepbound are changing what weight loss looks like for millions of people. Appetite decreases. Eating feels more manageable. Weight comes down in ways that once felt out of reach.
For many, this progress is life-changing. But there is an important part of the story that often receives less attention than the number on the scale. Studies continue to show that a significant portion of weight lost on GLP-1 medications comes from lean muscle mass, not just fat. Up to 39% of the weight lost from GLP-1 medication comes from lean muscle mass, not fat.¹
This matters because muscle is not extra weight. It supports metabolism, protects joints, and helps people stay strong and independent. Without a plan to protect it, weight loss on any of these medications can come at the expense of strength, mobility, and long-term success.
Why lean mass loss happens on GLP-1 medications
GLP-1 and GIP/GLP-1 medications reduce appetite and slow digestion. Eating less helps weight loss happen. At the same time, it often means people take in fewer nutrients, especially protein, unless they are intentional about it.
A recent academic study found that people using GLP-1 medications frequently consume less protein than their bodies need to maintain muscle.² When calorie intake drops and protein intake is too low, the body begins to break down muscle tissue for energy.
Movement patterns often change as well. Many people become less active after starting GLP-1 therapy. Lower appetite and lower energy can lead to fewer daily steps, more sitting, and less strength-based activity.
Less protein and less movement lead to muscle loss. Reviews published in The Lancet Diabetes & Endocrinology show that reductions in lean body mass are consistent across GLP-1 studies and that skeletal muscle is particularly vulnerable when movement is not part of the plan.³ This pattern explains why GLP-1 muscle loss is now one of the most important considerations for long-term outcomes.

How researchers study muscle loss during GLP-1 treatment
Much of what we know about muscle loss on GLP-1 medications comes from large clinical trials that followed people over many months and measured not just total weight loss, but how that weight was lost. These studies distinguish between:
- Fat mass, which most people want to lose
- Lean mass, which includes muscle and other non-fat tissue
By measuring both, researchers can see whether weight loss comes primarily from fat, or whether muscle is being lost as well.
What these GLP-1 trials measure well
- Total weight loss over time
- Changes in fat mass versus lean mass
- Patterns that occur when appetite is reduced without structured movement
What these GLP-1 trials do not measure
- How strong or functional someone feels day to day
- Whether muscle loss could have been prevented with guided movement
- Long-term joint health or future injury risk
This means the trials clearly show that muscle loss happens, but they do not reflect what is possible when medication is paired with strength-preserving movement.
What the research shows: GLP-1 drug by drug comparison
Much of what we know about muscle loss on GLP-1 medications comes from a series of large clinical studies known as the STEP trials. These studies followed thousands of people using semaglutide, the active ingredient in Ozempic and Wegovy, and measured not just total weight loss but how that weight was lost.
Importantly, researchers looked at changes in both fat mass and lean mass, which includes muscle. This distinction helps explain why some people feel weaker or lose strength during treatment, even when overall weight loss looks successful.
1. Ozempic (semaglutide for type 2 diabetes)
Ozempic contains semaglutide and was first studied in people with type 2 diabetes. Across clinical trials, researchers found that approximately 30 to 39 percent of total weight lost came from lean mass, not just fat.⁴ In the STEP 2 trial, participants experienced meaningful fat loss, but they also lost muscle. This finding matters because it shows muscle loss is not rare or limited to extreme weight reduction. It is a predictable outcome when appetite decreases and muscle is not actively protected.
2. Wegovy (semaglutide for weight management)
Wegovy uses the same active medication as Ozempic, but at a higher dose for weight management. In the STEP 1 and STEP 4 trials, researchers observed similar patterns. In some participants, lean mass made up close to 40 percent of the total weight lost.⁵ These studies help explain why some people feel weaker or lose strength during treatment, even when overall weight loss looks successful.
3. Mounjaro (tirzepatide)
Mounjaro is a dual GIP/GLP-1 medication and often leads to greater total weight loss than semaglutide. Early studies show lean mass loss in the range of 20 to 50 percent, consistent with other medications in this class.⁶ Direct comparisons are limited, but the underlying risk to muscle is clear.
4. Zepbound (tirzepatide for weight management)
Zepbound contains the same active medication as Mounjaro and is approved specifically for chronic weight management. Because the medication works the same way, the risk of lean mass loss is similar. This reinforces that the solution is not switching drugs, but addressing muscle loss directly.
Which GLP-1 medication is best for preserving muscle?
There is no strong evidence that one GLP-1 or GIP/GLP-1 medication is significantly better than the others at protecting muscle. Across trials, meaningful lean mass loss occurs when treatment is not paired with resistance-based movement and adequate nutrition.
The real differentiator is not the drug itself. The difference is what you do alongside it.
Without movement, all of these medications carry a risk of muscle loss. With structured strength-focused activity, people are more likely to protect muscle, support joint health, and sustain weight loss over time.
Protecting muscle is critical for strong long-term results
In a follow-up study of people who stopped semaglutide, participants regained about two-thirds of the weight they had lost within a year. Most of that weight returned as fat, not muscle.⁴
Muscle acts as your body’s engine and support system. Preserving it helps maintain metabolism, reduce joint strain, improve balance, and support long-term weight maintenance. Resistance-based movement is the only approach consistently shown to:
- Preserve muscle
- Maintain strength
- Protect joints
- Improve stability
- Support lasting weight loss
This is why guidance on preventing muscle loss during weight loss is becoming essential for anyone using GLP-1 medications.
Whether someone is taking Ozempic, Wegovy, Mounjaro, or Zepbound, the solution is the same: pair medication with structured, expert-guided movement.
Sword Move: the ideal partner program for all GLP-1 medications

Sword Move is a digital movement program designed to make muscle protection simple and accessible.
Members are paired with a Physical Health Specialist who holds a Doctor of Physical Therapy degree. Sessions are short, guided, and designed to be done at home. The Sword Move wearable (or you can use your own connected device )tracks activity automatically and plans evolve as strength improves, with regular check-ins to support consistency.
Get started with Sword Move for whole-body strength
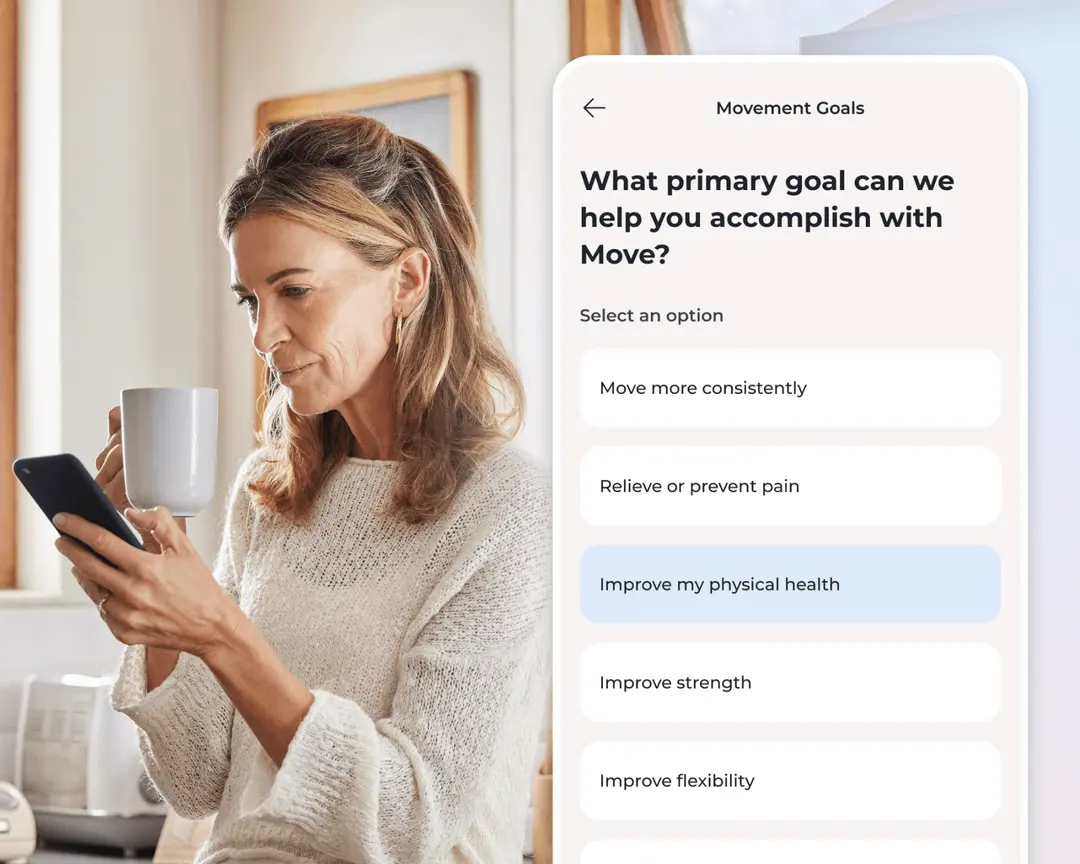
1. Tell us about you
We’ll learn about your goals, job type, lifestyle, and movement history.

2. Match with a Physical Health Specialist
Your dedicated Sword Move specialist will create a personalized plan just for you.

3. Receive your Move kit
You’ll get a free Move wearable and resistance bands delivered to your door.
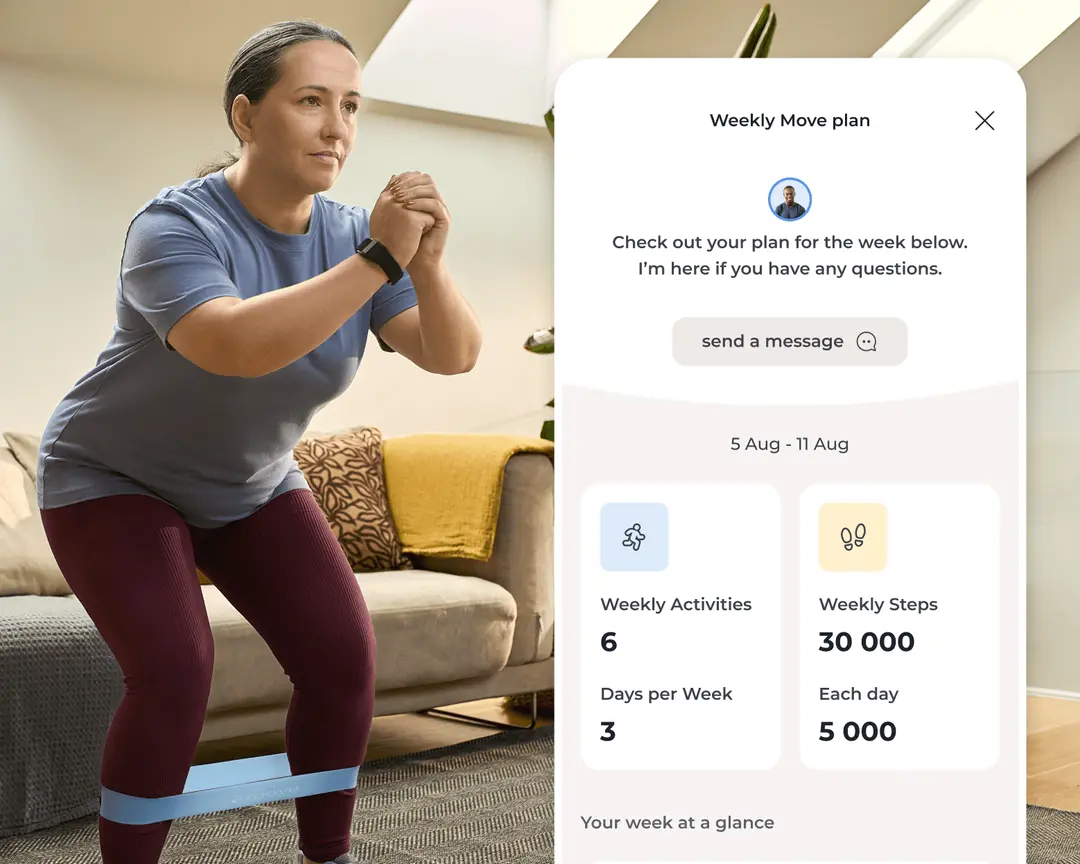
4. Start moving with your personalized plan
Pair your Move wearable and begin weekly goals built around your activity level, routines, and progress.
Start building strength from the comfort of home
GLP-1 medications can be powerful tools. But lasting results require more than appetite control alone. When weight loss is supported with structured movement, people are more likely to lose fat rather than muscle, protect their joints, maintain energy, and sustain results long term.
Sword Move is the ideal program designed to help you protect your muscle mass and develop the physical activity habits you need to keep the fat off well after your GLP-1 medication course is completed. The results of Move speak for themselves6.
69%
of members upgraded to healthy active status within 10-weeks of using Move4
91%
of members reported reported significant improvements after using Move
Sword’s Move program may already be covered in your health plan at no cost to you. Many US employers and health plans offer Move to their members. Check your eligibility now and you could get started right away.
About the author

Sword Editorial Team
Evidence-based healthcare insights